


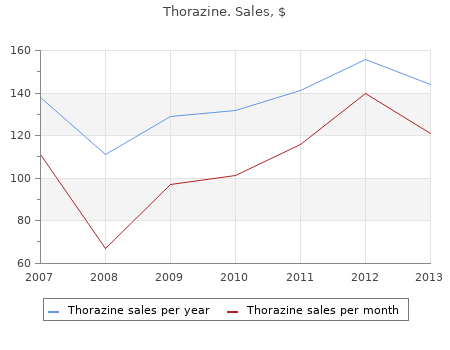
2017, Palm Beach Atlantic College, Mortis's review: "Thorazine 100 mg, 50 mg. Best Thorazine.".
COMPUTED TOMOGRAPHY Compared with MRI order 100 mg thorazine amex, CT is more rapid purchase 100 mg thorazine with mastercard, more avail- MAGNETIC RESONANCE IMAGING able, and less expensive and provides superior bone detail. The neu- ence of cardiac pacemakers, ferromagnetic aneurysm ral damage in as many as half of patients with cervi- clips, ferromagnetic cochlear implants, and intraocu- cal spine bone injuries, however, requires MRI for lar metallic foreign bodies. Open MRI may also be available for impingement but is inferior to MRI in detecting infec- these patients, but image quality is inferior. REFERENCES RADIONUCLIDE SCANNING Injection of technetium-99m-labeled phosphate com- 1. Morbidity Cost: National Estimates and plexes followed by a whole-body bone scan is a very Economic Determinants. These bone scans are useful in the Guideline Number 14: Acute Low Back Problems in Adults. Outpatient myelogra- is more sensitive as well as the test of choice in phy with fine-needle technique: An appraisal. AJR Am J patients with a strong suspicion of spinal metastases Roentgenol. Early MR demon- stration of spinal metastases in patients with normal radi- ographs and CT and radionuclide bone scans. DISCOGRAPHY Discography is the injection of contrast under fluoro- scopic guidance into the center of the nucleus pulpo- sus of an intervertebral disc. Smith, PhD Although it is the only imaging study that seeks to Jennifer A. Haythornthwaite, PhD establish a causal relationship between anatomic abnormalities and pain, discography is not often used in clinical practice. OVERVIEW: BIOPSYCHOSOCIAL MODEL OF PAIN ARTERIOGRAPHY The experience of pain is not equivalent to nocicep- tion, and tissue damage is only one of the factors Spinal arteriography is the intraarterial injection of influencing the experience of pain. Additional consideration should be given to (Note: Be careful to distinguish between interest and secondary gain and patient–provider interactions. Can you follow CRITICAL PSYCHOSOCIAL AND news stories in the newspaper or on television? Assessment The assessment of depression should focus on ques- Assessment Questions tions about interest in previously pleasurable activi- How frequently do you feel that you cannot stand the ties (eg, sexual activity, hobbies, time with family), pain?
Acute motion loss Gross deformity Traditional methods for treatment of chondral lesions Acute neurovascular deficit include the judicious use of nonsteroidal anti-inflam- Mechanical symptoms (catching cheap 50 mg thorazine otc, locking order 50 mg thorazine mastercard, sensation of a loose body) matory drugs combined with activity modification. Failed nonsurgical management greater than 3 months in duration Oral chondroprotective agents such as glucosamine Repeated giving way or complaints of instability 50 SECTION 1 GENERAL CONSIDERATIONS IN SPORTS MEDICINE SURGICAL MANAGEMENT quality and volume of repair tissue (fibrocartilage) is variable. These procedures are used in low demand patients with larger lesions (>2 cm2) or in higher Various surgical modalities exist for the treatment of demand patients with smaller lesions (<2 cm2). The goals are to reduce symptoms, and abrasion arthroplasty for several reasons: (1) it is improve joint congruence by restoring the articular sur- less destructive to the subchondral bone because it cre- face with the most normal tissue (i. Postoperative rehabilitation PALLIATIVE consists of nonweight bearing for 6 to 8 weeks and may include continuous passive motion (CPM) to improve Arthroscopic debridement and lavage is used to the extent and quality of the repair tissue. As MSTs are remove degenerative debris, cytokines, and proteases low-cost and relatively low-morbidity procedures, they that may contribute to cartilage breakdown. It is ide- remain the mainstay for the initial management of ally indicated in the patient with defect area less than small chondral lesions. Postoperative rehabilitation involves weight- bearing as tolerated and early strengthening exercises. RESTORATIVE In the absence of meniscal pathology, the results fol- lowing arthroscopic debridement are at best guarded. This restorative procedure results in the depth of chondrocyte death and cellular necrosis in hyaline-like cartilage which is believed to be superior the treated area and thus remains investigational. Postoperative reha- bilitation entails aggressive CPM and nonweight bear- ing for 6 weeks with a gradual increase to full-weight REPARATIVE bearing from 6 to 12 weeks. ACI is a costly procedure with a relatively lengthy recovery period and is most Marrow stimulating techniques (MST—microfracture, often used as a secondary procedure for the treatment abrasion arthroplasty, and subchondral drilling) involve of medium to larger focal chondral defects (>2 cm2). The resulting and articular cartilage which can be obtained from the TABLE 9-6 Surgical Management of Chondral Lesions PROCEDURE INDICATIONS OUTCOME Arthroscopic debridement Minimal symptoms, short-term relief Palliative and lavage Thermal chondroplasty Partial thickness defects, investigational Palliative (laser, radiofrequency energy) Marrow stimulating techniques Smaller lesions, persistent pain Reparative Autologous chondrocyte Small and large lesions with or without Restorative implantation subchondral bone loss Osteochondral autograft Smaller lesions, persistent pain Restorative Osteochondral allograft Larger lesions with subchondral bone loss Restorative CHAPTER 9 ARTICULAR CARTILAGE INJURY 51 TABLE 9-7 Results of Arthroscopic Debridement and Lavage AUTHOR N MEAN FOLLOW-UP RESULTS Owens et al, 2002 19 patients 24 months Fulkerson score 12 mos – 80. Osteochondral allograft can be used to treat larger ing the three-dimensional surface contour.
Physical symptoms are common in patients suffering from major depression [Lipowski cheap 100mg thorazine, 1990] cheap thorazine 100 mg overnight delivery. Approximately 60% of patients with depression report pain symptoms at the time of diagnosis [Magni et al. In the WHO’s data from 14 countries on five continents, 69% (range 45–95%) of patients with depression presented with only somatic symptoms, of which pain complaints were the most common [Simon et al. Half the depressed patients reported multiple unexplained somatic symptoms and 11% actively denied the psychological symptoms of depression. A survey of almost 19,000 Europeans found a 4-fold increase in the prevalence of chronic painful conditions in subjects with major depression [Ohayon and Schatzberg, 2003]. The presence of a depressive disorder has been demonstrated to increase the risk of developing chronic musculoskeletal pain, headache, and chest pain up to 3 years later [Leino and Magni, 1993; Magni et al. Even after 8 years, previously depressed patients remained twice as likely to develop chronic pain as the nondepressed. In a 15-year prospective study of workers in an industrial setting, initial depression symptoms predicted low back pain and a positive clinical back exam in men but not women [Leino and Magni, 1993]. Five years later, self-assessed depression at baseline was a significant predictor in the 25% of at-risk women who developed fibromyalgia [Forseth et al. Depression worsens other medical illnesses, interferes with their ongoing management, and amplifies their detrimental effects on health-related quality of life [Cassano and Fava, 2002; Gaynes et al. Depression in patients with chronic pain is associated with greater pain intensity, more pain persistence, less life control, more use of passive-avoidant coping strategies, noncompliance Perspectives on Pain and Depression 7 with treatment, application for early retirement, and greater interference from pain including more pain behaviors observed by others [Hasenbring et al. Primary care patients with musculoskeletal pain complicated by depression are significantly more likely to use medications daily, in combinations, and that include sedative-hypnotics [Mantyselka et al. In a study of over 15,000 employees who filed health claims, the cost of managing chronic conditions such as back problems was multiplied by 1. In a clinical trial of 1,001 depressed patients over age 60 years with arthritis, antidepressants and/or problem-solving oriented psychotherapy not only reduced depressive symptoms but also improved pain, functional status, and quality of life [Lin et al. Depression is a better predictor of disability than pain intensity and duration [Rudy et al.
Gift Certificate
